A long-term Microvasculature-On-A-Chip with unidirectional flow for vascular remodeling and Acute and Chronic toxicity studies

Why This Is Important

Challenges

Need
MIMETAS’ Answer
.svg)
Organ Model
A fully perfusable 3D microvascular network supported by stromal cells.
Features
MIMETAS developed OrganoAccess, an implementation-ready solution for building physiologically relevant human microvasculature models that combine scalability, reproducibility, and long-term survival for acute and chronic screening. OrganoAccess delivers a complete package: OrganoPlate Graft UniFlow (unidirectional-flow technology with 32 long-term perfusable microvascular networks per plate), a technology transfer package (including SOPs), and a starter reagents kit.
Intricate 3D vascular networks
Unidirectional flow
Long-term perfusability (up to 8+ weeks)
High reproducibility with minimal inter- experimental variation.
Scalable format (32 networks per plate)
Offering
Custom CRO services
OrganoAccess package
A Microvasculature-On-A-Chip model with unidirectional flow
Cardiovascular toxicity remains one of the leading causes of drug withdrawal1, yet current in vitro models lack the complexity and longevity needed for chronic safety studies. To address this, we developed a self-assembling microvascular model in the OrganoPlate® Graft 32 UniFlow. Human endothelial cells are co-cultured with stromal fibroblasts in a fibrin matrix, forming an intricate, perfusable 3D vascular network that closely mimics the architecture of human microvasculature. The extracellular matrix and stromal cells act as a natural scaffold, providing the structural and biological support that keeps vessels stable and functional over 8 weeks. Despite this complexity, the model supports 32 independent chips in a pump-free standard plate format, retaining full compatibility with automated imaging and liquid-handling workflows (Figure 1).
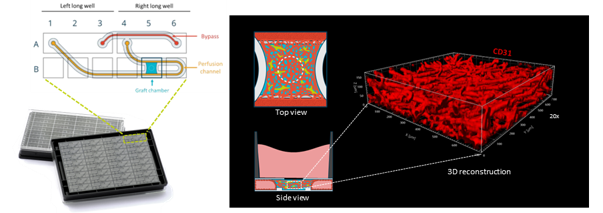
Figure 1. Microvasculature-on-a-Chip in the OrganoPlate® 32 UF.
(C) Top and side views of the gel compartment, where fibrin-embedded endothelial cells and fibroblasts are seeded to form a microvascular network. (D) Three-dimensional reconstruction of immunofluorescent CD31-positive vessels (Day 15 of culture) demonstrating the formation of an intricate 3D vascular network.
Reproducibility and longevity of microvascular networks
A key requirement for industrial adoption is that models perform consistently across experiments and operators and retain long-term perfusability. Representative images of vascular networks from five independent experiments carried out by three different operators show consistent network architecture regardless of who ran the assay (Figure 2A). Vascular networks not only remained fully perfusable but continued to mature, with vessel density increasing over time for at least 57 days (Figure 2B), a remarkable longevity well beyond the timescales of conventional in vitro models.
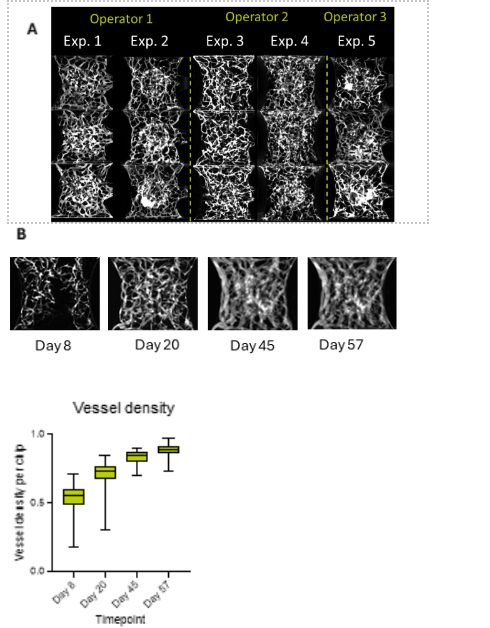
Figure 2. Reproducibility and long-term stability of microvascular networks.
(A) Representative images of vascular networks from five independent experiments performed by three operators. Networks were perfused with 150 kDa FITC–dextran at day 20 to enable morphological comparison. (B) Microvascular networks were maintained for up to 57 days in culture without signs of degeneration, as indicated by a progressive increase in vessel density (n = 75).Real-time TEER monitoring measurements showing concentration-dependent impairment of epithelial barrier integrity during treatment and subsequent recovery after compound withdrawal.
Modelling inflammatory responses with immune cell perfusion
The microvascular model is fully compatible with immune cell perfusion. Endothelial response to inflammatory stimuli is recapitulated by a marked increase in PBMC adhesion to the endothelium.(Figure 3A). Beyond adhesion, immune cells also undergo transendothelial migration into the ECM compartment (yellow arrow), making this a complete model for studying inflammation-driven endothelium–immune cell interactions (Figure 3B).er expression enable highly reliable and physiologically relevant compound transport across the gut barrier (Figure 3B).
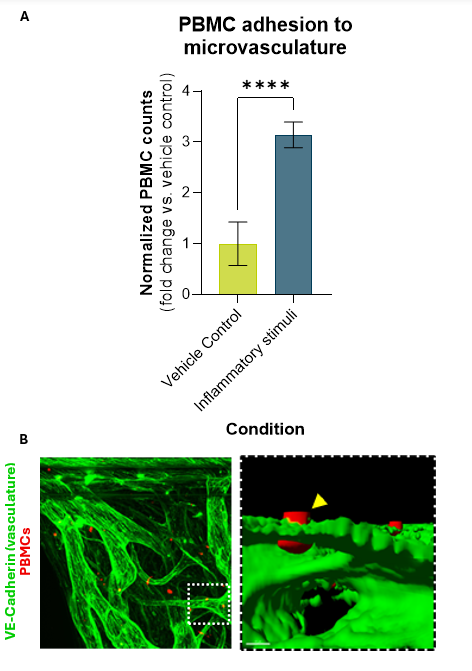
Figure 3. PBMC adhesion and transendothelial migration.
(A) Normalized levels of PBMC adhesion in the microvasculature 24 h after inflammatory stimulation (n = 6). (B) Maximum intensity projection of PBMCs (red) in the microvascular network (green) and three-dimensional reconstruction showing transendothelial migration of a PBMC into the extracellular matrix compartment (yellow arrow).
Modeling acute and chronic vascular toxicity
To demonstrate compatibility with both acute and chronic toxicological studies, vascular networks were exposed to Sorafenib, a tyrosine kinase inhibitor widely used in cancer treatment and known for its vascular off-target effects. Following 72-hour acute exposure, no significant impact on vascular perfusion was observed at either 1 or 10 µM (Figure 4). This is consistent with the clinical picture where in healthy, mature vasculature, TKI-induced vascular rarefaction develops gradually, as seen in patients where capillary bed toxicity emerges over time2. This is reflected in chronic exposure over 21 days where 10 µM Sorafenib not only abrogated the increase in perfusable vessel density seen in control networks, but drove it below baseline (Figure 4B). These results highlight that the model is compatible with both acute and chronic compound exposure, and that long-term experiments are essential to capture the slow-onset vascular responses that short-term assays entirely miss.
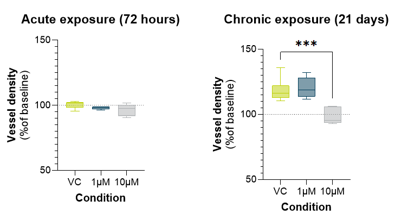
Figure 4. Effects of Sorafenib on vascular network perfusability.
Change in perfusable vessel density following acute (72 h) and chronic (21 days) exposure to 1 or 10 µM Sorafenib (n = 6–7).
Summary
- Physiologically Relevant Microvasculature: Intricate, perfusable 3D vascular networks supported by ECM and stromal cells, closely mimicking human microvasculature architecture.
- Reproducible and Long-Lived: Consistent network formation across experiments and operators, with vessel density increasing and perfusability maintained for at least 57 days.
- Compatible with Immune Cell Perfusion: Recapitulates endothelial inflammatory responses, including PBMC adhesion and transendothelial migration following TNF-α priming.
- Acute and Chronic Toxicity Assessment: Detects compound-induced vascular effects invisible to short-term assays, enabling the long-term exposure studies that chronic cardiovascular toxicity requires.
References
- Laverty, H. G., Benson, C., Cartwright, E. J., Cross, M. J., Garland, C., Hammond, T., ... & Valentin, J. P. (2011). How can we improve our understanding of cardiovascular safety liabilities to develop safer medicines?. British journal of pharmacology, 163(4), 675-693.
- Coschignano MA, De Ciuceis C, Agabiti-Rosei C, Brami V, Rossini C, Chiarini G, Malerba P, Famà F, Cosentini D, Muiesan ML, Salvetti M, Petelca A, Capellini S, Arnoldi C, Nardin M, Grisanti S, Rizzoni D, Berruti A and Paini A (2021) Microvascular Structural Alterations in Cancer Patients Treated With Antiangiogenic Drugs. Front. Cardiovasc. Med. 8:651594. doi: 10.3389/fcvm.2021.651594


Selected Resources
.avif)

